Those of us who have made it our goal to breed better Mastiffs and have invested years of involvement in this breed, often try to inform buyers why health testing is important. Now, health testing involves more than just having your Vet give your dog a health exam. It's a process of certifying and clearing a dog through medical test and exams. Often referred as "OFAing" a dog. X-rays of hips, elbows, shoulders, and patellas are taken and sent in to be reviewed and graded for a rating. Blood or cheek swabs are submitted for DNA testing to clear dogs of certain diseases, or sent to approved labs for panel tests. The results of these tests are then listed online in the OFA site (offa.org) so that dog owners may be able research health results.
Until you have a beloved pet develop a chronic or acute life altering illness, you may not understand why it's so important not to breed dogs that are not affected with certain diseases. Watching your pet's health slowly decline due to a preventable disease can definitely make you a believer in health testing. Does it cost more for a puppy from health tested parents and lines? Yes, it does. However, to cost of treating hip dysplasia in a puppy less than a year can be upwards of $4-6000 for surgeries. Why have a puppy that goes blind from PRA when we have had the test to DNA clear parents for over 10 years? Why buy a puppy from a parent with thyroid or cardiac issues?
When you have a parent with a diseases (affected) or if both parents are carriers (carry 1 clear gene and 1 affected gene) you risk getting a puppy that may be affected with the disease. You may have saved money on your purchase price, but increase Vet medical cost will certainly mount in total cost over time. I tell people you can pay up front or pay later. Never buy a puppy from lines that have not been health tested.
Due to the hard work of caring and ethical breeders, we have increased the overall quality of health in our breed. OFA has a listing of the stat results of health testing for each breed, and the results are encouraging.
Here are just a few of the results for Mastiffs up through December 2017.
PRA- 99,3% are clear, 0.7% are abnormal.
CMR-1-75.8% are clear, 22.2% are carries, and 2.0 % are abnormal.
Cardiac-99.1% are clear, and 0.4% are abnormal
Advanced Cardiac-98.6% are clear
Cystinuria- 97.2% are clear, 0.7% are abnormal.
Degenerative Myelopathy- 82.7% are clear, 16.5% are carriers, and 0.8% are abnormal.
Elbow Dysplasia-84.3% are clear, 15.4% are abnormal
Eyes (CERF)-97.6% clear, 2.4% are abnormal
Hip Dysplasia-76.3% are clear, and 20.7% are abnormal
Patellas-99.7% are clear.
Shoulders-95.9% are clear
Thyroid-87.0% are clear, and 2.7% are abnormal, and 10.2% are equivocal.
Von Willebrands- 100.0% are clear.
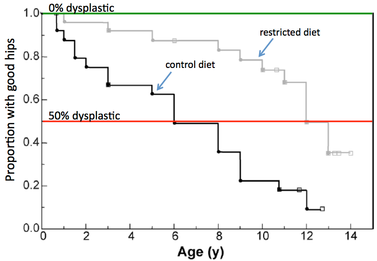
As a breeder, I have seen a marked increase in the improvement in the overall health of our breed, and I am greatly encouraged. As we have improved the general health of our breed, we have also increased our longevity. The dogs bred from health tested lines are now living longer and healthier lives.
Many breeders have also added temperament testing to their dogs--CGC, obedience titles, agility, therapy certifications all point to a dog that had a stable and correct temperament. Always look for these titles and proof of certifications in your puppy's lines.
Be an educated and informed buyer, research the common health issues in your puppy's breed. Ask your puppy's breeder if they health test, and ask for the parent's registered names of registry number so you can look up the health testing on the OFA site. Look to see if there has been consistent health testing in the preceding generations. If a pattern of affected dogs is noted--make sure your puppy is clear of those health issues before you buy and take it home.
Even when we health test and breed from multiple generations of health and temperament tested dogs, issues can occur. Ethical breeders will guarantee the health and temperament of their puppy. With that guarantee comes peace of mind for puppy owners. These same breeders will also be there for their puppy owners to answer questions and be a information resource. Your $500.00 Craigslist puppy will not come with those benefits.
Don't buy the first puppy you find online. Don't buy a puppy out of pity or emotional response because you feel it needs to "be rescued". Be an informed and educated puppy buyer so that you can bring into your family a Dog that is healthy in body and mind.
Cathy C Arney
KioKee Mastiffs
Hickory, NC
NCkiokeemastiffs@charter.net